
Shoulder Dystocia
Home : : Specialities : : Shoulder Dystocia
Shoulder Dystocia
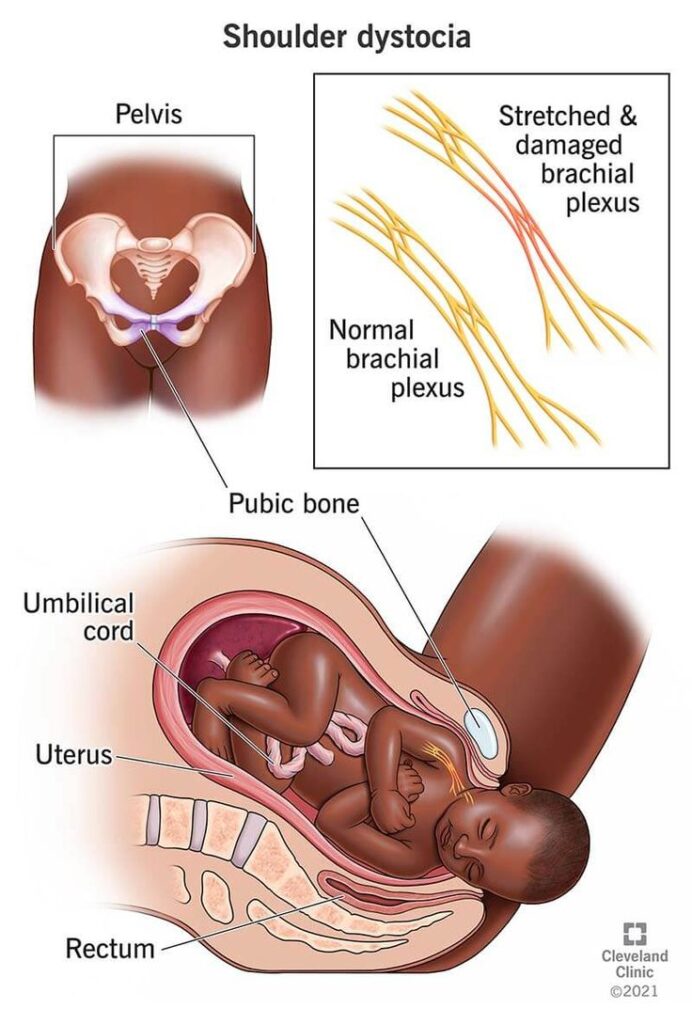
Shoulder dystocia is a childbirth complication in which one or both of the baby’s shoulders become stuck behind the mother’s pelvic bone during delivery. This condition is considered an obstetric emergency because it can lead to serious complications for both the mother and the baby if not managed promptly and effectively.
Symptoms of Shoulder Dystocia
Causes shoulder dystocia
Fetal Macrosomia: This is one of the most common risk factors for shoulder dystocia. It occurs when the baby is larger than average (often weighing more than 4,000 grams or 8 pounds, 13 ounces).
Maternal Diabetes: Mothers with diabetes, particularly gestational diabetes, are at a higher risk of having larger babies, which can increase the risk of shoulder dystocia.
Prolonged Labor: A slow or prolonged labor can increase the likelihood of shoulder dystocia, as the baby’s head may descend further into the birth canal, making it more difficult for the shoulders to pass through.
Previous Shoulder Dystocia: If a woman has had a previous delivery complicated by shoulder dystocia, she is at a higher risk of experiencing it again in subsequent pregnancies.
Maternal Obesity: Women with a higher body mass index (BMI) are more likely to have larger babies and an increased risk of shoulder dystocia.
Abnormal Fetal Position: Babies in certain abnormal positions, such as breech or face presentation, may be more prone to shoulder dystocia.
Maternal Diabetes: Mothers with diabetes, particularly gestational diabetes, are at a higher risk of having larger babies, which can increase the risk of shoulder dystocia.
Prolonged Labor: A slow or prolonged labor can increase the likelihood of shoulder dystocia, as the baby’s head may descend further into the birth canal, making it more difficult for the shoulders to pass through.
Previous Shoulder Dystocia: If a woman has had a previous delivery complicated by shoulder dystocia, she is at a higher risk of experiencing it again in subsequent pregnancies.
Maternal Obesity: Women with a higher body mass index (BMI) are more likely to have larger babies and an increased risk of shoulder dystocia.
Abnormal Fetal Position: Babies in certain abnormal positions, such as breech or face presentation, may be more prone to shoulder dystocia.
Treatment of Shoulder Dystocia
McRoberts Maneuver: This is the first-line maneuver, where the mother’s legs are sharply flexed towards her abdomen. This action may help reposition the baby’s shoulders.
Suprapubic Pressure: Pressure is applied to the mother’s abdomen just above the pubic bone to help dislodge the baby’s anterior shoulder.
Woods’ Corkscrew Maneuver: If the above maneuvers do not work, a healthcare provider may attempt to rotate the baby’s shoulders to allow for easier delivery.
Zavanelli Maneuver: In extreme cases, when other methods fail, the baby’s head may be pushed back into the birth canal, and a cesarean section may be performed.
Episiotomy: In some cases, an episiotomy (a surgical cut to enlarge the vaginal opening) may be performed to facilitate the delivery of the baby.
Suprapubic Pressure: Pressure is applied to the mother’s abdomen just above the pubic bone to help dislodge the baby’s anterior shoulder.
Woods’ Corkscrew Maneuver: If the above maneuvers do not work, a healthcare provider may attempt to rotate the baby’s shoulders to allow for easier delivery.
Zavanelli Maneuver: In extreme cases, when other methods fail, the baby’s head may be pushed back into the birth canal, and a cesarean section may be performed.
Episiotomy: In some cases, an episiotomy (a surgical cut to enlarge the vaginal opening) may be performed to facilitate the delivery of the baby.